

|
For healthcare practitioners and substance misuse case workers, writing accurate case notes is an essential skill and a crucial part of their daily practice. “If it’s not written down, it didn’t happen” is an often repeated maxim that workers are regularly reminded of. It is important to remember that a client’s case notes could be read out in court. What are Case Notes? Case notes are a record of interactions, observations and actions relating to a particular client which are recorded chronologically. For clients engaging in drug / alcohol treatment, case notes are a vital element of the support that is offered as they help practitioners maintain a continuity of care for that client, provide details of other agencies / professionals involved in that person’s care and are the main source of information for enquiries and investigations. |
 |
|
Alongside a written account of the client contact, case notes can also include:
The format of case notes can vary, depending on the setting within which they’re written – the format of a social worker’s case note may differ from that of a psychologist, for example. That said, it is important for each service to adopt their own defined process and approach. |
|
Why are case notes important and what are the challenges? One of the challenges faced by services where a standard approach to case note writing has not been followed – or indeed, where no standard has been set by the organisation – is that the lack of consistency can make it difficult to effectively monitor what work is being delivered, what a client’s presenting risks are and the details of the plan put in place to minimise these risks. According to research, record-keeping techniques have an impact on client results, such that poor case notes can lead to poor decision-making and negative client outcomes (see Preston-Shoot 2003, Cumming et al. 2007) Common errors within case note writing can include:
By following a set format – or template – workers can easily avoid these mistakes and build upon their case note writing skills.
|
|
What solutions can help overcome these challenges? In most healthcare organisations we are increasingly seeing how, by following a standard case note template, services are able to minimise the risk of inaccurate record keeping which in turn helps inform key treatment decisions. One method many services adopt around standardising their case notes is the SOAP format. The SOAP format frames each case note within four sections:
By fostering communication among healthcare providers and aiding them in remembering each client’s case better, the benefit of case notes that adhere to the SOAP template is an improvement in the quality and continuity of client services (Kettenbach, 1995). Professionals may detect, prioritise, and track their client’s presenting issues using the SOAP format, which can then be managed more effectively and a continuous evaluation of the client’s progress and treatment actions becomes more visible. Examples A freedom of information request is one of the real-world scenarios that can be used to illustrate the advantages of using a standard format. It is simpler for patients to get the precise information they need and easier for them to comprehend what they are reading if all healthcare organisations use a uniform structure and procedure. |
| How can ILLY help?
At ILLY, we continuously develop and improve our systems so that all users can continue to support their clients effectively, at the same time introducing time-saving measures for workers that frequently have to manage large caseloads.
|
||
| The Case Note Template functionality is one such time-saving measure – a configurable setting which allows services to tailor the format of their case notes to their own agreed standard, ensuring that all client contacts are recorded in a methodical and comprehensive style. Users also have the option of saving a draft version of a case note – this helps workers to quickly record the key outputs of their client contacts which they can then update later. A full audit history of all case notes in CarePath is accessible from within the client record. | 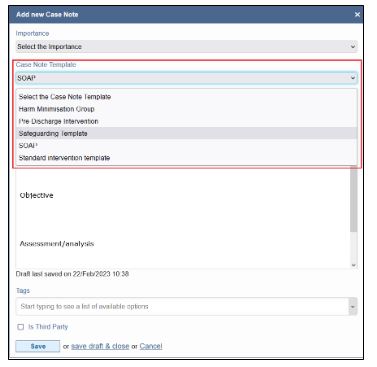 |
|
|
By improving the consistency of case note writing we can support services maintain continuity of care and ensure client records remain a valuable source of information. If you have any questions or would like to find out more, please get in touch with our Client Services Team and we’ll be happy to help. |
||
|
+44 (0)20 4566 5727 |